Clearly, with hindsight, doing nothing would have been better that doing "something, anything" mostly stupid things. Doing the right thing: Protect and vaccinate the most vulnerable in priority... and stop there, would have been even better. But don't expect to read that anywhere in the news, anytime soon. The Medias have been hijacked by private interest who now completely control the narrative. The solution to bad policies will be more of those policies as always. Necessarily. Until the system breaks...
Via Swiss Policy Research,
Austria,
one of the most repressive European countries during the coronavirus
pandemic, has recently overtaken Sweden in terms of total covid
mortality, showing that almost all government interventions have been
ineffective and unjustified.
Throughout the coronavirus pandemic, Austria has been one of the most repressive European
countries, implementing several lockdowns, school closures,
far-reaching mask mandates and even an N95/FFP2 mask mandate,
record-setting mass PCR testing and contact tracing, as well as early
“vaccine passports”. Austria was also the first Western country to
impose a “lockdown for the unvaccinated” and the first Western country
to announce a general “vaccine mandate”.
In contrast, Sweden has
widely been regarded, or indeed criticized, as the least repressive
Western country during the coronavirus pandemic, imposing no lockdowns,
no elementary school closures, no mask mandates, no “vaccine passport”,
and very limited testing and contact tracing compared to Austria and most other Western countries.
And yet, in December 2021, Austria overtook Sweden in
terms of total covid mortality (see chart above). This comes after
Austria had reached, in late November, the highest seven-day covid infection rate in the world. The European average covid mortality had already overtaken Swedish covid mortality back in March 2021.
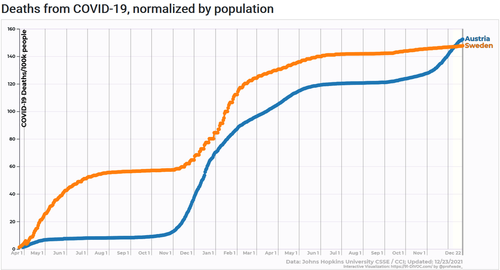
Total covid mortality: Sweden vs. Austria (JHU/CSSE)
But can Nordic Sweden and Alpine Austria really be compared in a legitimate way? Indeed, they can. To begin with, their population size is quite similar (10.4 million in Sweden vs. 9.0 million in Austria). While the median age in Sweden is slightly lower than in Austria (41.1 vs. 44.4 years; perhaps due to more immigration), the Swedish life expectancy is actually somewhat higher than in Austria (82.4 vs. 81.6 years).
Interestingly, the population weighted density, which takes urbanization into account, is somewhat higher in Sweden than in Austria (2724 vs. 2191, see map below). Obesity rates are very similar in Sweden and in Austria (20.6% vs. 20.1%). ICU capacity is significantly higher in Austria than in Sweden (5.3 vs. 1.9 beds per 1000 people).
In
fact, total covid mortality in Austria and Sweden has reached the same
level precisely because the two countries are so similar in terms of
demographic and health factors. In both countries, the covid population fatality rate (PFR) has reached about 0.15% and is limited primarily to people over 70 years of age (the median age of covid deaths is about 83 years in both countries).
But is it fair to call December 2021 the “judgment day”? Indeed it is, because Sweden has already crossed the “pandemic finish line” and was the first Western country to see the return of influenza,
which had been displaced by the coronavirus since March of 2020. Of
course, the novel coronavirus will not disappear from Sweden or from
anywhere else, and Sweden will certainly see future coronavirus waves,
but Sweden has achieved a high population infection rate (about 60% to 75%) and has entered the endemic phase.
Thus,
the fact that Austria has now overtaken Sweden in terms of total covid
mortality really means that almost every single government intervention
in Austria – and almost everywhere else – has been entirely ineffective
from an epidemiological and medical perspective, while having caused
almost unprecedented social and economic harm.
In particular, it means that lockdowns, school closures, mask mandates, N95/FFP2 mask mandates, mass PCR testing and “contact tracing”, as well as “vaccine passports”, have been entirely ineffective and unjustified as interventions to “combat the pandemic”.
Of note, this is not just “post-hoc knowledge”: with the exception of school closures (which are effective against influenza), it had long been known that
all of these “interventions”, including masks and contact tracing, are
ineffective against respiratory virus epidemics. Concerning masks, the
question is not if they are effective in theory or in some lab
experiment, but if they make any difference in the real world – and the answer is no.
In fact, in terms of all-cause excess mortality, Austria had surpassed Sweden already several months ago:
total pandemic excess mortality currently is 17% in Austria vs. 11% in
Sweden. This is primarily because many Swedish deaths happened earlier
in the pandemic (in the spring of 2020) and most covid victims were very
old (median age of 83); thus, by September 2020, Sweden recorded its
lowest mortality in history. (Nevertheless, claims that Sweden has no or
almost no excess mortality are based on an incorrect calculation method; there is no “Swedish miracle”).
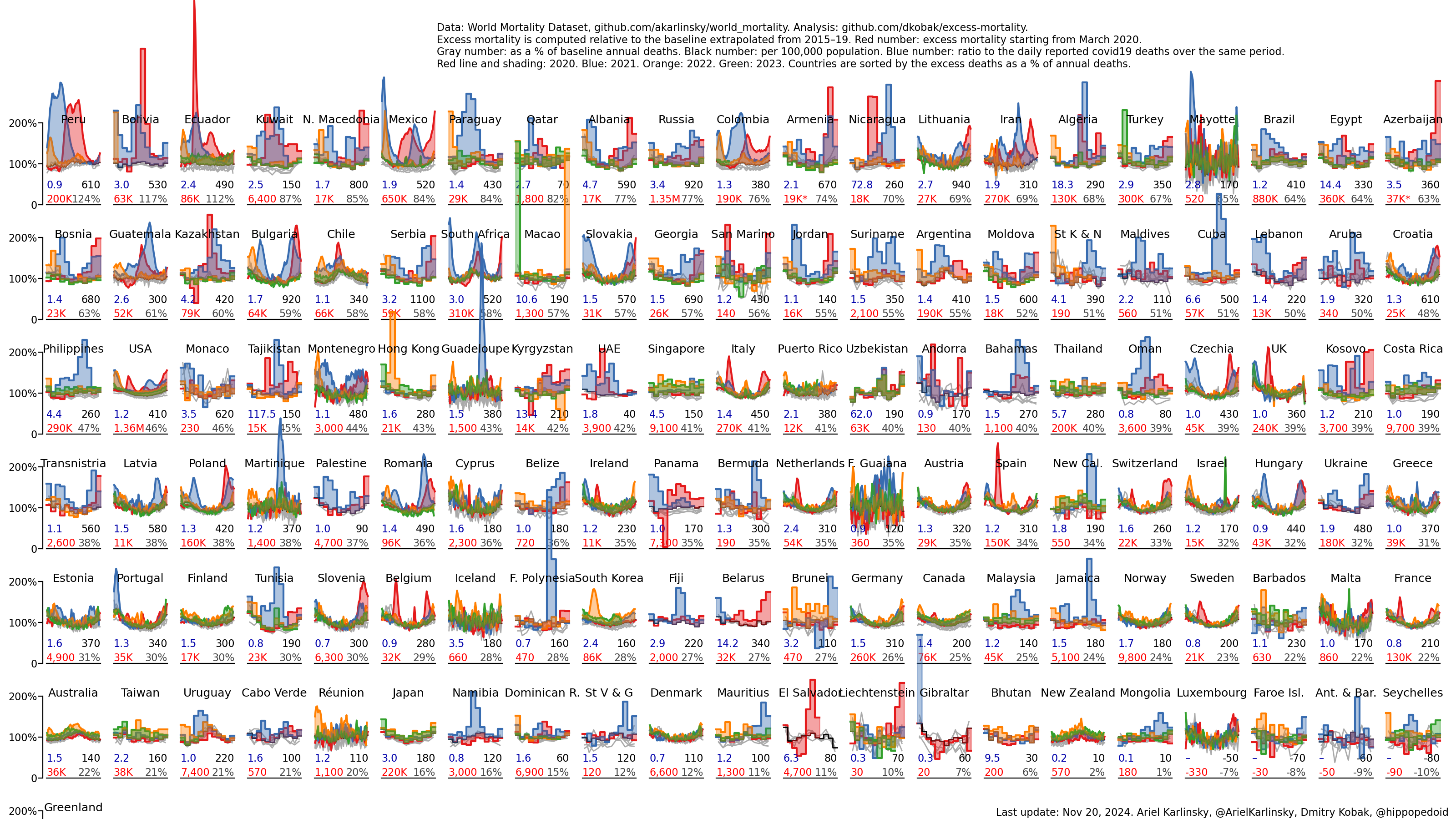
The same result has been observed in many other regions throughout the world: In Eastern Europe, Belarus has recorded an average regional excess mortality despite
almost no interventions at all; in Latin America, excess mortality in
Brazil has been higher than in Chile and Argentina, but lower than in Peru, Bolivia, Ecuador, Mexico, Colombia and Paraguay; in Asia, lockdowns in India, Indonesia or the Philippines were horrific failures affecting 800 million children.
There was only one situation in which lockdowns were a rational intervention: as a preemptive measure in support of early border controls.
This situation applied primarily to some islands, such as Australia,
New Zealand and Iceland, and possibly to Norway, Finland, Denmark and
parts of China (more on these countries below).
Critics of the Swedish approach have often argued that Sweden should only be compared to “its neighbors”.
If one compares Sweden to all of its neighbors in the region – Norway,
Finland, Denmark, but also Poland and the Baltic states – Sweden again
shows an average covid mortality: Poland, Latvia and Lithuania are much higher, Estonia is similar, while Denmark, Finland and Norway are much lower.
But
some critics of Sweden insist on comparing Sweden only to Denmark,
Finland and Norway. These critics would like to imply that Sweden is a
high mortality outlier, when in reality, it is Denmark, Finland and
Norway which are the true outliers, having by far the lowest covid
mortality rates among Western countries. But why is this?
It is
not, as critics of Sweden would like to imply, because these countries
had particularly strict measures. In fact, for the most part, their
“stringency index” was even lower than in Sweden, and of course also lower than in repressive countries like Austria.
Instead, three explanations seem plausible.
First, Denmark, Finland and Norway imposed early border controls and
could avoid a major unexpected wave in the spring of 2020. “Early” here
is a relative term and always depends on when the coronavirus reaches a
certain country. Due to the timing of its winter holidays, the
Stockholm area unknowingly imported the
coronavirus directly from early covid hotspots in Alpine skiing resorts
near Italy, which was not the case in other Nordic countries or even in
other regions of Sweden. (In the famous case of Uruguay in South
America, the first covid wave hit not until November 2020).
Second, and in the same context, other Nordic countries imposed preemptive lockdowns in support of early border controls that really may have helped disrupt
early infections. But a lockdown is ‘preemptive’ only as long as there
have been either no confirmed infections at all or only a very small
number of infections that can still be contained without aerosolizing
the virus.
Third, and most fundamentally, Norway and Finland have by far the lowest population weighted densities in Europe (910
in Norway and 986 in Finland, vs. 2724 in Sweden and 6785 in Britain;
see the map below), which may have slowed the spread of covid.
In fact, in Western Europe, there is a striking correlation between
population weighted density – which may influence the speed of virus
transmission and the amplitude of infection waves – and covid mortality
per country (see map below). This correlation does not apply, however,
to Denmark, which has a low covid mortality but an average population
weighted density (3434).
At the global level,
high population weighted density might help explain strong covid waves
in Britain, Spain and Italy, Turkey, South America (including Mexico)
and South Africa, but not (so far) in Japan, Canada, Australia and New
Zealand. Low population weighted density could help explain the slow
spread of the coronavirus in Norway, Finland, Indochina, and parts of
Black Africa (see map below).
Coming back to the comparison between Sweden and Austria, one factor that worked against Austria was the failure of covid vaccines:
if covid vaccines had provided strong long-term protection, Austria
could have avoided the very high covid mortality in the winter of
2021/22 (see chart above). On the other hand, in the spring of 2020,
even optimists hadn’t expected covid vaccines becoming available before
autumn 2021.
The failure of covid vaccines is also a major problem
for low-covid countries like Norway, Finland, Australia, New Zealand
and China, which now are in a very uncertain position.
While all of the interventions imposed by Austria and other repressive countries failed, are there any potentially effective interventions that have not been adopted?
A few options may be mentioned.
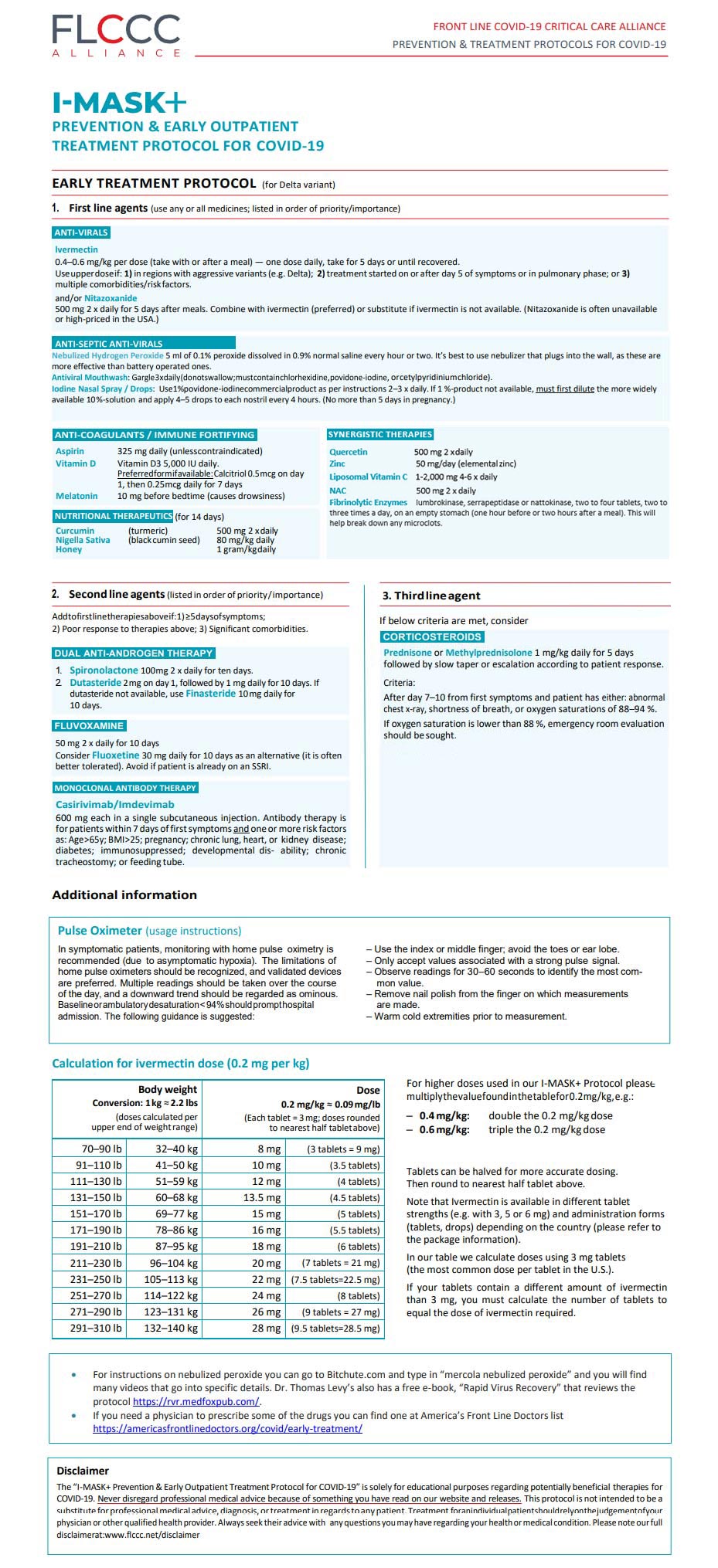
First, research and use of repurposed early treatment drugs should have been a major priority to reduce hospitalizations (especially given the uncertainties regarding vaccine protection).
Second, dedicated covid hospital facilities should
have been created to avoid widespread in-hospital transmission (in some
countries, including Sweden, the UK and the US, such facilities were
indeed created, but they remained largely unused).
Third, given their low covid risk, offering voluntary, medically supervised live virus infection to children and young healthy adults may
have made sense to rapidly build up a natural immunity shield, protect
high-risk groups (including parents), and ensure smooth education.
Fourth, while masks have been a complete failure (as was already known before the pandemic), indoor ventilation to
prevent aerosol transmission might have been one of the most effective
interventions (with >99% of all transmission occurring indoors). Then
again, living rooms and class rooms cannot be turned into airplane
cabins.
Fifth, the media should have supported
the calm management of the pandemic, fostering social cohesion and
mindfulness, instead of inciting panic and hysteria. The many
“dashboards” and “live tickers” may well have been counterproductive.
Sixth, we may have to recognize that societies with a life expectancy of over 80 years and obesity rates of over 20% are inherently susceptible to events like the coronavirus pandemic.
Needless to say, most Western health authorities have not yet acknowledged that
their entire approach to the pandemic has been a complete failure. In a
typical move, the Austrian health minister in early December claimed
that the most recent Austrian lockdown had been effective in breaking
the winter wave, but independent analysts quickly pointed out that
infections had decreased simultaneously in neighboring countries without a lockdown.
In conclusion,
the comparison of Austria and Sweden conclusively shows that a calm,
low-intervention, almost business-as-usual approach to the pandemic has
been best. In contrast, highly irrational strategies, such as “zero
covid” and “no covid”, have caused unprecedented social, political and
economic damage at an almost civilizational scale.







{kind=link}