ALL the data about Covid, as complete as can be to understand "the pandemic".
(I will keep this article for reference.)
By Kit Knightly on Offguardian - Article
Here are key facts and sources about the alleged “pandemic”, that will help you get a grasp on what has happened to the world since January 2020, and help you enlighten any of your friends who might be still trapped in the New Normal fog (click links to skip):
“Covid deaths” – Lockdowns – PCR Tests – “asymptomatic infection” – Ventilators – Masks – Vaccines – Deception & Foreknowledge
*
PART I: “COVID DEATHS” & MORTALITY
1. The survival rate of “Covid” is over 99%. Government medical experts went out of their way to underline, from the beginning of the pandemic, that the vast majority of the population are not in any danger from Covid.
Almost all studies on the infection-fatality ratio (IFR) of Covid have returned results between 0.04% and 0.5%. Meaning Covid’s survival rate is at least 99.5%.
*
2. There has been NO unusual excess mortality. The press has called 2020 the UK’s “deadliest year since world war two”, but this is misleading because it ignores the massive increase in the population since that time. A more reasonable statistical measure of mortality is Age-Standardised Mortality Rate (ASMR):
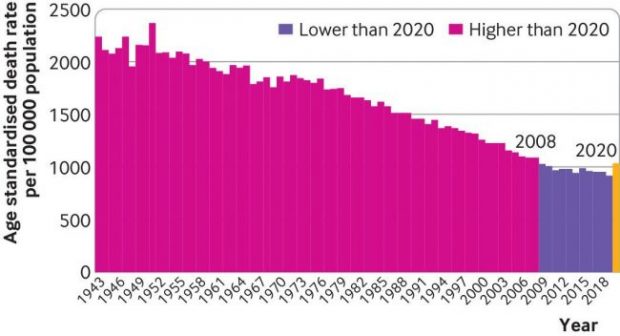
By this measure, 2020 isn’t even the worst year for mortality since 2000, In fact since 1943 only 9 years have been better than 2020.
Similarly, in the US the ASMR for 2020 is only at 2004 levels:
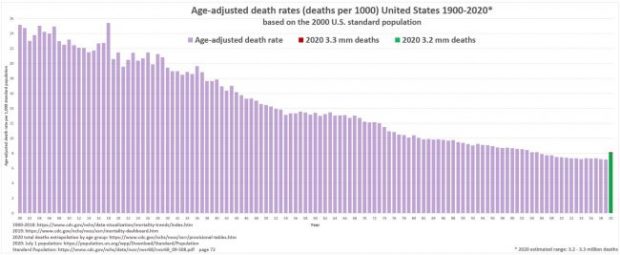
For a detailed breakdown of how Covid affected mortality across Western Europe and the US click here. What increases in mortality we have seen could be attributable to non-Covid causes [facts 7, 9 & 19].
*
3. “Covid death” counts are artificially inflated. Countries around the globe have been defining a “Covid death” as a “death by any cause within 28/30/60 days of a positive test”.
Healthcare officials from Italy, Germany, the UK, US, Northern Ireland and others have all admitted to this practice:
Removing any distinction between dying of Covid, and dying of something else after testing positive for Covid will naturally lead to over-counting of “Covid deaths”. British pathologist Dr John Lee was warning of this “substantial over-estimate” as early as last spring. Other mainstream sources have reported it, too.
Considering the huge percentage of “asymptomatic” Covid infections [14], the well-known prevalence of serious comorbidities [fact 4] and the potential for false-positive tests [fact 18], this renders the Covid death numbers an extremely unreliable statistic.
*
4. The vast majority of covid deaths have serious comorbidities. In March 2020, the Italian government published statistics showing 99.2% of their “Covid deaths” had at least one serious comorbidity.
These included cancer, heart disease, dementia, Alzheimer’s, kidney failure and diabetes (among others). Over 50% of them had three or more serious pre-existing conditions.
This pattern has held up in all other countries over the course of the “pandemic”. An October 2020 FOIA request to the UK’s ONS revealed less than 10% of the official “Covid death” count at that time had Covid as the sole cause of death.
*
5. Average age of “Covid death” is greater than the average life expectancy. The average age of a “Covid death” in the UK is 82.5 years. In Italy it’s 86. Germany, 83. Switzerland, 86. Canada, 86. The US, 78, Australia, 82.
In almost all cases the median age of a “Covid death” is higher than the national life expectancy.
As such, for most of the world, the “pandemic” has had little-to-no impact on life expectancy. Contrast this with the Spanish flu, which saw a 28% drop in life expectancy in the US in just over a year. [source]
*
6. Covid mortality exactly mirrors the natural mortality curve. Statistical studies from the UK and India have shown that the curve for “Covid death” follows the curve for expected mortality almost exactly:
The risk of death “from Covid” follows, almost exactly, your background risk of death in general.
The small increase for some of the older age groups can be accounted for by other factors.[facts 7, 9 & 19]
*
7. There has been a massive increase in the use of “unlawful” DNRs. Watchdogs and government agencies have reported huge increases in the use of Do Not Resuscitate Orders (DNRs) over the last twenty months.
In the US, hospitals considered “universal DNRs” for any patient who tested positive for Covid, and whistleblowing nurses have admitted the DNR system was abused in New York.
In the UK there was an “unprecdented” rise in “illegal” DNRs for disabled people, GP surgeries sent out letters to non-terminal patients recommending they sign DNR orders, whilst other doctors signed “blanket DNRs” for entire nursing homes.
A study done by Sheffield Univerisity found over one-third of all “suspected” Covid patients had a DNR attached to their file within 24 hours of hospital admission.
Blanket use of coerced or illegal DNR orders could account for any increases in mortality in 2020/21.[Facts 2 & 6]
*
Part II: Lockdowns
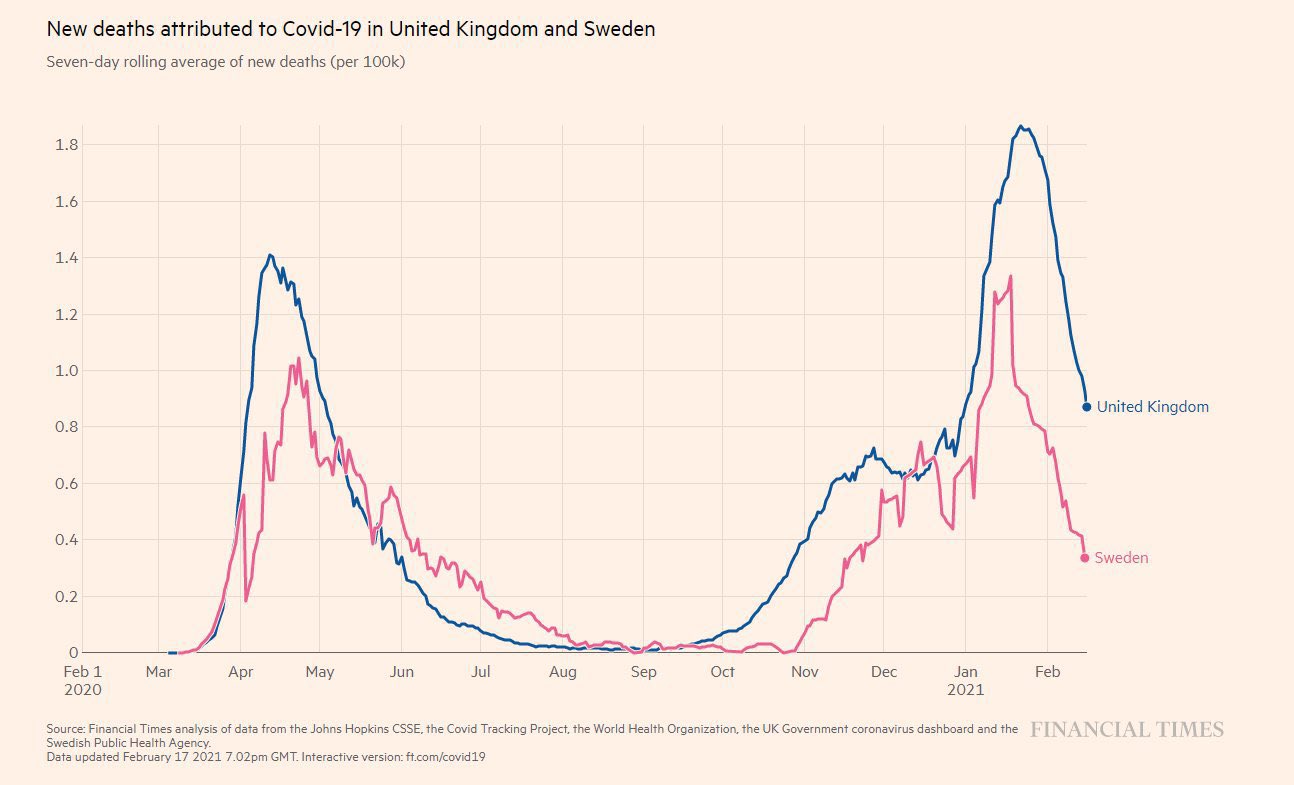
8. Lockdowns do not prevent the spread of disease. There is little to no evidence lockdowns have any impact on limiting “Covid deaths”. If you compare regions that locked down to regions that did not, you can see no pattern at all.
*
9. Lockdowns kill people. There is strong evidence that lockdowns – through social, economic and other public health damage – are deadlier than the “virus”.
Dr David Nabarro, World Health Organization special envoy for Covid-19 described lockdowns as a “global catastrophe” in October 2020:
We in the World Health Organization do not advocate lockdowns as the primary means of control of the virus[…] it seems we may have a doubling of world poverty by next year. We may well have at least a doubling of child malnutrition […] This is a terrible, ghastly global catastrophe.”
A UN report from April 2020 warned of 100,000s of children being killed by the economic impact of lockdowns, while tens of millions more face possible poverty and famine.
Unemployment, poverty, suicide, alcoholism, drug use and other social/mental health crises are spiking all over the world. While missed and delayed surgeries and screenings are going to see increased mortality from heart disease, cancer et al. in the near future.
The impact of lockdown would account for the small increases in excess mortality [Facts 2 & 6]
*
10. Hospitals were never unusually over-burdened. the main argument used to defend lockdowns is that “flattening the curve” would prevent a rapid influx of cases and protect healthcare systems from collapse. But most healthcare systems were never close to collapse at all.
In March 2020 it was reported that hospitals in Spain and Italy were over-flowing with patients, but this happens every flu season. In 2017 Spanish hospitals were at 200% capacity, and 2015 saw patients sleeping in corridors. A paper JAMA paper from March 2020 found that Italian hospitals “typically run at 85-90% capacity in the winter months”.
In the UK, the NHS is regularly stretched to breaking point over the winter.
As part of their Covid policy, the NHS announced in Spring of 2020 that they would be “re-organizing hospital capacity in new ways to treat Covid and non-Covid patients separately” and that “as result hospitals will experience capacity pressures at lower overall occupancy rates than would previously have been the case.”
This means they removed thousands of beds. During an alleged deadly pandemic, they reduced the maximum occupancy of hospitals. Despite this, the NHS never felt pressure beyond your typical flu season, and at times actually had 4x more empty beds than normal.
In both the UK and US millions were spent on temporary emergency hospitals that were never used.
*
Part III: PCR Tests
11. PCR tests were not designed to diagnose illness. The Reverse-Transcriptase Polymerase Chain Reaction (RT-PCR) test is described in the media as the “gold standard” for Covid diagnosis. But the Nobel Prize-winning inventor of the process never intended it to be used as a diagnostic tool, and said so publicly:
PCR is just a process that allows you to make a whole lot of something out of something. It doesn’t tell you that you are sick, or that the thing that you ended up with was going to hurt you or anything like that.”
*
12. PCR Tests have a history of being inaccurate and unreliable. The “gold standard” PCR tests for Covid are known to produce a lot of false-positive results, by reacting to DNA material that is not specific to Sars-Cov-2.
A Chinese study found the same patient could get two different results from the same test on the same day. In Germany, tests are known to have reacted to common cold viruses. A 2006 study found PCR tests for one virus responded to other viruses too. In 2007, a reliance on PCR tests resulted in an “outbreak” of Whooping Cough that never actually existed. Some tests in the US even reacted to the negative control sample.
The late President of Tanzania, John Magufuli, submitted samples goat, pawpaw and motor oil for PCR testing, all came back positive for the virus.
As early as February of 2020 experts were admitting the test was unreliable. Dr Wang Cheng, president of the Chinese Academy of Medical Sciences told Chinese state television “The accuracy of the tests is only 30-50%”. The Australian government’s own website claimed “There is limited evidence available to assess the accuracy and clinical utility of available COVID-19 tests.” And a Portuguese court ruled that PCR tests were “unreliable” and should not be used for diagnosis.
You can read detailed breakdowns of the failings of PCR tests here, here and here.
*
13. The CT values of the PCR tests are too high. PCR tests are run in cycles, the number of cycles you use to get your result is known as your “cycle threshold” or CT value. Kary Mullis said: “If you have to go more than 40 cycles[…]there is something seriously wrong with your PCR.”
The MIQE PCR guidelines agree, stating: “[CT] values higher than 40 are suspect because of the implied low efficiency and generally should not be reported,” Dr Fauci himself even admitted anything over 35 cycles is almost never culturable.
Dr Juliet Morrison, virologist at the University of California, Riverside, told the New York Times: Any test with a cycle threshold above 35 is too sensitive…I’m shocked that people would think that 40 [cycles] could represent a positive…A more reasonable cutoff would be 30 to 35″.
In the same article Dr Michael Mina, of the Harvard School of Public Health, said the limit should be 30, and the author goes on to point out that reducing the CT from 40 to 30 would have reduced “covid cases” in some states by as much as 90%.
The CDC’s own data suggests no sample over 33 cycles could be cultured, and Germany’s Robert Koch Institute says nothing over 30 cycles is likely to be infectious.
Despite this, it is known almost all the labs in the US are running their tests at least 37 cycles and sometimes as high as 45. The NHS “standard operating procedure” for PCR tests rules set the limit at 40 cycles.
Based on what we know about the CT values, the majority of PCR test results are at best questionable.
*
14. The World Health Organization (Twice) Admitted PCR tests produced false positives. In December 2020 WHO put out a briefing memo on the PCR process instructing labs to be wary of high CT values causing false positive results:
when specimens return a high Ct value, it means that many cycles were required to detect virus. In some circumstances, the distinction between background noise and actual presence of the target virus is difficult to ascertain.
Then, in January 2021, the WHO released another memo, this time warning that “asymptomatic” positive PCR tests should be re-tested because they might be false positives:
Where test results do not correspond with the clinical presentation, a new specimen should be taken and retested using the same or different NAT technology.
*
15. The scientific basis for Covid tests is questionable. The genome of the Sars-Cov-2 virus was supposedly sequenced by Chinese scientists in December 2019, then published on January 10th 2020. Less than two weeks later, German virologists (Christian Drosten et al.) had allegedly used the genome to create assays for PCR tests.
They wrote a paper, Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR, which was submitted for publication on January 21st 2020, and then accepted on January 22nd. Meaning the paper was allegedly “peer-reviewed” in less than 24 hours. A process that typically takes weeks.
Since then, a consortium of over forty life scientists has petitioned for the withdrawal of the paper, writing a lengthy report detailing 10 major errors in the paper’s methodology.
They have also requested the release of the journal’s peer-review report, to prove the paper really did pass through the peer-review process. The journal has yet to comply.
The Corman-Drosten assays are the root of every Covid PCR test in the world. If the paper is questionable, every PCR test is also questionable.
*
Part IV: “Asymptomatic infection”
16. The majority of Covid infections are “asymptomatic”. From as early as March 2020, studies done in Italy were suggesting 50-75% of positive Covid tests had no symptoms. Another UK study from August 2020 found as much as 86% of “Covid patients” experienced no viral symptoms at all.
It is literally impossible to tell the difference between an “asymptomatic case” and a false-positive test result.
*
17. There is very little evidence supporting the alleged danger of “asymptomatic transmission”. In June 2020, Dr Maria Van Kerkhove, head of the WHO’s emerging diseases and zoonosis unit, said:
From the data we have, it still seems to be rare that an asymptomatic person actually transmits onward to a secondary individual,”
A meta-analysis of Covid studies, published by Journal of the American Medical Association (JAMA) in December 2020, found that asymptomatic carriers had a less than 1% chance of infecting people within their household. Another study, done on influenza in 2009, found:
…limited evidence to suggest the importance of [asymptomatic] transmission. The role of asymptomatic or presymptomatic influenza-infected individuals in disease transmission may have been overestimated…”
Given the known flaws of the PCR tests, many “asymptomatic cases” may be false positives.[fact 14]
*
Part V: Ventilators
18. Ventilation is NOT a treatment for respiratory viruses. Mechanical ventilation is not, and never has been, recommended treatment for respiratory infection of any kind. In the early days of the pandemic, many doctors came forward questioning the use of ventilators to treat “Covid”.
Writing in The Spectator, Dr Matt Strauss stated:
Ventilators do not cure any disease. They can fill your lungs with air when you find yourself unable to do so yourself. They are associated with lung diseases in the public’s consciousness, but this is not in fact their most common or most appropriate application.
German Pulmonologist Dr Thomas Voshaar, chairman of Association of Pneumatological Clinics said:
When we read the first studies and reports from China and Italy, we immediately asked ourselves why intubation was so common there. This contradicted our clinical experience with viral pneumonia.
Despite this, the WHO, CDC, ECDC and NHS all “recommended” Covid patients be ventilated instead of using non-invasive methods.
This was not a medical policy designed to best treat the patients, but rather to reduce the hypothetical spread of Covid by preventing patients from exhaling aerosol droplets.
*
19. Ventilators killed people. Putting someone on a ventilator who is suffering from influenza, pneumonia, chronic obstructive pulmonary disease, or any other condition which restricts breathing or affects the lungs, will not alleviate any of those symptoms. In fact, it will almost certainly make it worse, and will kill many of them.
Intubation tubes are a source of potential a infection known as “ventilator-associated pneumonia”, which studies show affects up to 28% of all people put on ventilators, and kills 20-55% of those infected.
Mechanical ventilation is also damaging to the physical structure of the lungs, resulting in “ventilator-induced lung injury”, which can dramatically impact quality of life, and even result in death.
Experts estimate 40-50% of ventilated patients die, regardless of their disease. Around the world, between 66 and 86% of all “Covid patients” put on ventilators died.
According to the “undercover nurse”, ventilators were being used so improperly in New York, they were destroying patients’ lungs:
This policy was negligence at best, and potentially deliberate murder at worst. This misuse of ventilators could account for any increase in mortality in 2020/21 [Facts 2 & 6]
*
Part VI: Masks
20. Masks don’t work. At least a dozen scientific studies have shown that masks do nothing to stop the spread of respiratory viruses.
One meta-analysis published by the CDC in May 2020 found “no significant reduction in influenza transmission with the use of face masks”.
Another study with over 8000 subjects found masks “did not seem to be effective against laboratory-confirmed viral respiratory infections nor against clinical respiratory infection.”
There are literally too many to quote them all, but you can read them: [1][2][3][4][5][6][7][8][9][10] Or read a summary by SPR here.
While some studies have been done claiming to show mask do work for Covid, they are all seriously flawed. One relied on self-reported surveys as data. Another was so badly designed a panel of experts demand it be withdrawn. A third was withdrawn after its predictions proved entirely incorrect.
The WHO commissioned their own meta-analysis in the Lancet, but that study looked only at N95 masks and only in hospitals. [For full run down on the bad data in this study click here.]
Aside from scientific evidence, there’s plenty of real-world evidence that masks do nothing to halt the spread of disease.
For example, North Dakota and South Dakota had near-identical case figures, despite one having a mask-mandate and the other not:
In Kansas, counties without mask mandates actually had fewer Covid “cases” than counties with mask mandates. And despite masks being very common in Japan, they had their worst flu outbreak in decades in 2019.
*
21. Masks are bad for your health. Wearing a mask for long periods, wearing the same mask more than once, and other aspects of cloth masks can be bad for your health. A long study on the detrimental effects of mask-wearing was recently published by the International Journal of Environmental Research and Public Health
Dr. James Meehan reported in August 2020 he was seeing increases in bacterial pneumonia, fungal infections, facial rashes .
Masks are also known to contain plastic microfibers, which damage the lungs when inhaled and may be potentially carcinogenic.
Childen wearing masks encourages mouth-breathing, which results in facial deformities.
People around the world have passed out due to CO2 poisoning while wearing their masks, and some children in China even suffered sudden cardiac arrest.
*
22. Masks are bad for the planet. Millions upon millions of disposable masks have been used per month for over a year. A report from the UN found the Covid19 pandemic will likely result in plastic waste more than doubling in the next few years., and the vast majority of that is face masks.
The report goes on to warn these masks (and other medical waste) will clog sewage and irrigation systems, which will have knock on effects on public health, irrigation and agriculture.
A study from the University of Swansea found “heavy metals and plastic fibres were released when throw-away masks were submerged in water.” These materials are toxic to both people and wildlife.
*
Part VII: Vaccines
23. Covid “vaccines” are totally unprecedented. Before 2020 no successful vaccine against a human coronavirus had ever been developed. Since then we have allegedly made 20 of them in 18 months.
Scientists have been trying to develop a SARS and MERS vaccine for years with little success. Some of the failed SARS vaccines actually caused hypersensitivity to the SARS virus. Meaning that vaccinated mice could potentially get the disease more severely than unvaccinated mice. Another attempt caused liver damage in ferrets.
While traditional vaccines work by exposing the body to a weakened strain of the microorganism responsible for causing the disease, these new Covid vaccines are mRNA vaccines.
mRNA (messenger ribonucleic acid) vaccines theoretically work by injecting viral mRNA into the body, where it replicates inside your cells and encourages your body to recognise, and make antigens for, the “spike proteins” of the virus. They have been the subject of research since the 1990s, but before 2020 no mRNA vaccine was ever approved for use.
*
24. Vaccines do not confer immunity or prevent transmission. It is readily admitted that Covid “vaccines” do not confer immunity from infection and do not prevent you from passing the disease onto others. Indeed, an article in the British Medical Journal highlighted that the vaccine studies were not designed to even try and assess if the “vaccines” limited transmission.
The vaccine manufacturers themselves, upon releasing the untested mRNA gene therapies, were quite clear their product’s “efficacy” was based on “reducing the severity of symptoms”.
*
25. The vaccines were rushed and have unknown longterm effects. Vaccine development is a slow, laborious process. Usually, from development through testing and finally being approved for public use takes many years. The various vaccines for Covid were all developed and approved in less than a year. Obviously there can be no long-term safety data on chemicals which are less than a year old.
Pfizer even admit this is true in the leaked supply contract between the pharmaceutical giant, and the government of Albania:
the long-term effects and efficacy of the Vaccine are not currently known and that there may be adverse effects of the Vaccine that are not currently known
Further, none of the vaccines have been subject to proper trials. Many of them skipped early-stage trials entirely, and the late-stage human trials have either not been peer-reviewed, have not released their data, will not finish until 2023 or were abandoned after “severe adverse effects”.
*
26. Vaccine manufacturers have been granted legal indemnity should they cause harm. The USA’s Public Readiness and Emergency Preparedness Act (PREP) grants immunity until at least 2024.
The EU’s product licensing law does the same, and there are reports of confidential liability clauses in the contracts the EU signed with vaccine manufacturers.
The UK went even further, granting permanent legal indemnity to the government, and any employees thereof, for any harm done when a patient is being treated for Covid19 or “suspected Covid19”.
Again, the leaked Albanian contract suggests that Pfizer, at least, made this indemnity a standard demand of supplying Covid vaccines:
Purchaser hereby agrees to indemnify, defend and hold harmless Pfizer […] from and against any and all suits, claims, actions, demands, losses, damages, liabilities, settlements, penalties, fines, costs and expenses
*
Part VIII: Deception & Foreknowledge
27. The EU was preparing “vaccine passports” at least a YEAR before the pandemic began. Proposed COVID countermeasures, presented to the public as improvised emergency measures, have existed since before the emergence of the disease.
Two EU documents published in 2018, the “2018 State of Vaccine Confidence” and a technical report titled “Designing and implementing an immunisation information system” discussed the plausibility of an EU-wide vaccination monitoring system.
These documents were combined into the 2019 “Vaccination Roadmap”, which (among other things) established a “feasibility study” on vaccine passports to begin in 2019 and finish in 2021:
This report’s final conclusions were released to the public in September 2019, just a month before Event 201 (below).
*
28. A “training exercise” predicted the pandemic just weeks before it started. In October 2019 the World Economic Forum and Johns Hopkins University held Event 201. This was a training exercise based on a zoonotic coronavirus starting a worldwide pandemic. The exercise was sponsored by the Bill and Melinda Gates Foundation and GAVI the vaccine alliance.
The exercise published its findings and recommendations in November 2019 as a “call to action”. One month later, China recorded their first case of “Covid”.
*
29. Since the beginning of 2020, the Flu has “disappeared”. In the United States, since February 2020, influenza cases have allegedly dropped by over 98%.
It’s not just the US either, globally flu has apparently almost completely disappeared.
Meanwhile, a new disease called “Covid”, which has identical symptoms and a similar mortality rate to influenza, is apparently affecting all the people normally affected by the flu.
*
30. The elite have made fortunes during the pandemic. Since the beginning of lockdown the wealthiest people have become significantly wealthier. Forbes reported that 40 new billionaires have been created “fighting the coronavirus”, with 9 of them being vaccine manufacturers.
Business Insider reported that “billionaires saw their net worth increase by half a trillion dollars” by October 2020.
Clearly that number will be even bigger by now.



{kind=link}
{kind=link}
No comments:
Post a Comment